

In a Phase 3 Paloma-III study of Pfizer’s CDK4/6 inhibitor (Ibrance – palbociclib) and an estrogen receptor antagonist (Faslodex – fulvestrant), patients receiving the combination had significantly prolonged progression-free survival than women with breast cancer who received Faslodex, alone.
The study randomized 521 pre/perimenopausal and postmenopausal women with hormone receptor-positive, HER2-negative metastatic breast cancer whose disease had progressed during or after endocrine therapy to receive Faslodex in combination with Ibrance or placebo. An interim analysis showed that PFS was 9.2 months in patients given Ibrance plus Fasodex, versus 3.8 months for those who received Faslodex plus placebo.
In February, Ibrance was granted accelerated approval by FDA when combined with an aromatase inhibitor (Femara – letrozole) in patients with HR+ (hormone receptor positive) / HER-2 negative breast cancer. Ibrance has now shown activity in combination with anti-estrogen therapy in patients with metastatic breast cancer both in the front-line and after progression following endocrine therapy.
What is the mechanism of action of Ibrance?
Ibrance (palbociclib) is an inhibitor of cyclin-dependent kinase (CDK) 4 and 6. Cyclin D1 and CDK4/6 are downstream of signaling pathways which lead to cellular proliferation. In vitro, palbociclib reduced cellular proliferation of estrogen receptor (ER)-positive breast cancer cell lines by blocking progression of the cell from G1 into S phase of the cell cycle. Treatment of breast cancer cell lines with the combination of palbociclib and antiestrogens leads to decreased retinoblastoma protein (Rb) phosphorylation resulting in reduced E2F expression and signaling and increased growth arrest compared to treatment with each drug alone. In vitro treatment of ER-positive breast cancer cell lines with the combination of palbociclib and antiestrogens leads to increased cell senescence, which was sustained for up to 6 days following drug removal. In vivo studies using a patient-derived ER-positive breast cancer xenograft model demonstrated that the combination of palbociclib and letrozole increased the inhibition of Rb phosphorylation, downstream signaling and tumor growth compared to each drug alone.
Virtually all mitogenic signals to the cell are processed through CDK4/6 – it is truly the central molecule that governs pRb phosphorylation status up through the R-point transition.
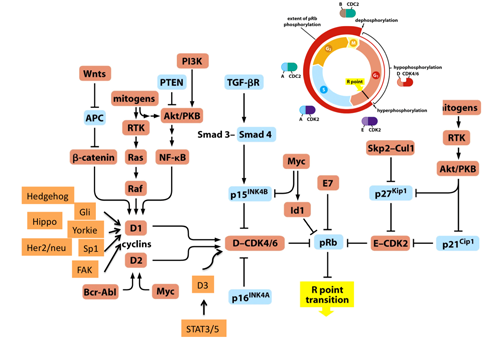
Rb blocks cell cycle progression in G1 by binding E2F transcription factors. In order to enter S phase, cells must sequentially activate CDK4/6 and CDK2. These kinases are expressed throughout the cell cycle, but are only activated upon complex formation with their corresponding cyclins. During early G1 phase, mitogenic signals trigger activation of the CDK4/6-cyclin D complex, which partially deactivates Rb by phosphorylation. Subsequently released E2F factors mediate expression of pro-proliferative genes including cyclin E and Cdc25A. This transfers cells past the restriction (R) point, which commits for S-phase entry. Activation of the CDK2-cyclin E complex results in hyperphosphorylation of Rb and fully releases E2F. The expression of further E2F target genes, as cyclin A, facilitates progression through S phase. Upstream inhibitors, including members of the Ink4 and Cip/Kip families, inhibit the mitogenic action of CDKs. ARF and p53 can block cell cycle progression via p21Cip1. ARF, alternate reading frame; CDK, cyclin-dependent kinase; Rb, retinoblastoma. http://www.nature.com/mt/journal/v20/n5/fig_tab/mt20122f1.html
What is anti-estrogen therapy?
Anti-estrogen therapy involves blocking the production, binding, or signaling of estrogen in cancer cells. Estrogen is a mitogenic growth factor – disrupting the production or effective signaling of estrogen deprives cells of signals to divide.
Molecular action of estrogen: E: Estrogen Receptor, ERE: estrogen responsible elements, P450 Scc: P450 side chain cleavage enzyme, CYP17: 17β-hydroxylase, 3β-HDS: denotes 3β-hydroxysteroid dehydrogonase, DHEA: dehydroepiandrosterone, 17-KSR: 17-ketosteroid reductase, 17β-HDS: 17β hydroxysteroid dehydrogonase.
If you have taken Faslodex with success the first round of 3 months and poor response 2nd round of four months would adding the Ibrance to it and continuing the treatment help
faslodex be helpful